
The Case for
CIPN Treatment
The Case for CIPN Treatment
Lahara Bio is developing Low Intensity Vibration (LIV) as a non-invasive, non-pharmacologic therapy designed to prevent and treat chemotherapy-induced peripheral neuropathy.
Lahara Bio is developing Low Intensity Vibration (LIV) as a non-invasive, non-pharmacologic therapy designed to prevent and treat chemotherapy-induced peripheral neuropathy.
The Unmet Need
A crisis across the care continuum
A crisis across the care continuum
CIPN compromises patient healthcare at multiple levels
CIPN compromises patient healthcare at multiple levels
FOR PATIENTS
FOR PATIENTS
Permanent nerve damage that outlasts cancer treatment. Numbness, burning pain, and loss of function in hands and feet. Over 3 million Americans live with chronic CIPN today.
Permanent nerve damage that outlasts cancer treatment. Numbness, burning pain, and loss of function in hands and feet. Over 3 million Americans live with chronic CIPN today.
450k+
450k+
new cases per year
new cases per year
new cases per year
FOR ONCOLOGISTS
FOR ONCOLOGISTS
CIPN forces impossible choices. When neuropathy becomes severe, oncologists must reduce or stop chemotherapy, compromising cancer outcomes to manage a side effect they cannot reliably treat.
CIPN forces impossible choices. When neuropathy becomes severe, oncologists must reduce or stop chemotherapy, compromising cancer outcomes to manage a side effect they cannot reliably treat.
#1
#1
#1
reason for dose reduction
reason for dose reduction
reason for dose reduction
FOR PAYERS
FOR PAYERS
No prevention, no effective treatment, and enormous downstream costs. ER visits, chronic pain management, physical therapy, disability claims, all because no intervention exists.
No prevention, no effective treatment, and enormous downstream costs. ER visits, chronic pain management, physical therapy, disability claims, all because no intervention exists.
>$17k
>$17k
>$17k
excess healthcare costs per patient
excess healthcare costs per patient
excess healthcare costs per pt
Taxanes
60-70%
develop CIPN
Paclitaxel, Docetaxel
Stabilizes microtubules toinduce cell death
Platinums
40-80%
develop CIPN
Cisplatin, Oxaloplatin
dose-dependent DNA damage
Vinca Alkyloids
40-60%
develop CIPN
Vincristine, vinblastine
Axonal transport disruption
Antibody Drug Conjugates
30-60%
develop CIPN
Vedotin containing ADCs
Microtubule stabilization
Proteasome Inhibitors
30-60%
develop CIPN
Bortezomib
Inducing protein accumulation
Immunomodulators
20-40%
develop CIPN
Thalidomide, lenalidomide
Cumulative nerve damage
Taxanes
60-70%
develop CIPN
Paclitaxel, Docetaxel
Stabilizes microtubules toinduce cell death
Platinums
40-80%
develop CIPN
Cisplatin, Oxaloplatin
dose-dependent DNA damage
Vinca Alkyloids
40-60%
develop CIPN
Vincristine, vinblastine
Axonal transport disruption
Antibody Drug Conjugates
30-60%
develop CIPN
Vedotin containing ADCs
Microtubule stabilization
Proteasome Inhibitors
30-60%
develop CIPN
Bortezomib
Inducing protein accumulation
Immunomodulators
20-40%
develop CIPN
Thalidomide, lenalidomide
Cumulative nerve damage
Treatment Landscape
Existing therapies fall short
Existing therapies fall short
PHARMACOLOGIC
Duloxetine
Off-Label, Modest Evidence
The only guideline-recommended option, but only for painful CIPN. Duloxetine has not been shown effective at treating sensory symtptoms (numbness/tingling) or functional decline. It's benefit is modest even for pain management.
WHY IT FAILS
Treats pain only; does not restore nerve function or prevent damage
Modest efficacy: NNT of ~5 for 30% pain reduction
Additional side effect burden (nausea, fatigue, dizziness) in already-burdened patients
No impact on the underlying neuropathic progression
Used off-label for this indication; not FDA-approved for CIPN
PHARMACOLOGIC
Gabapentin
Off-Label, No Evidence
Widely prescribed despite no controlled evidence supporting its use in CIPN. Clinical guidelines explicitly recommend against gabapentinoids for this indication.
WHY IT FAILS
No randomized controlled trial has demonstrated efficacy in CIPN
ASCO guidelines recommend against use for CIPN prevention or treatment
Sedation and cognitive dulling impair quality of life during chemotherapy
Risk of dependence and withdrawal with prolonged use
PHYSICAL
Cryotherapy
Unproven
Ice gloves and compression socks applied during infusion to reduce drug delivery to extremities. Logistically difficult, uncomfortable, and supported by limited and conflicting data.
WHY IT FAILS
Uncomfortable for patients already enduring multi-hour infusion sessions
Limited and conflicting clinical evidence across studies
Requires in-clinic administration during every infusion cycle
No standardized protocols; wide variation in technique
Only addresses extremities, not systemic nerve damage
PHYSICAL
T.E.N.S. Therapy
Symptom Management Only
Transcutaneous electrical nerve stimulation provides temporary pain modulation by disrupting nerve signaling. It does not address nerve damage and has minimal evidence specific to CIPN.
WHY IT FAILS
Masks pain signals without treating the underlying nerve injury
Effects are temporary; symptoms return when stimulation stops
Very limited clinical evidence specific to chemotherapy-induced neuropathy
Requires patient compliance with daily electrode placement during treatment
BEHAVIORAL
Exercise
Impractical for Cancer Patients
The only approach with genuine neuroprotective evidence through mechanobiological pathways. But chemotherapy patients are too fatigued, immunosuppressed, and deconditioned to exercise at therapeutic levels.
WHY IT FAILS
Proven neuroprotective through multi-pathway mechanical signaling
Activates conserved mechanosensitive signaling pathways to protect neurons
Chemotherapy-related fatigue prevents adherence in 60-80% of patients
Not feasible at therapeutic intensity during chemotherapy cycles
PHARMACOLOGIC
Duloxetine
Off-Label, Modest Evidence
The only guideline-recommended option, but only for painful CIPN. Duloxetine has not been shown effective at treating sensory symtptoms (numbness/tingling) or functional decline. It's benefit is modest even for pain management.
WHY IT FAILS
Treats pain only; does not restore nerve function or prevent damage
Modest efficacy: NNT of ~5 for 30% pain reduction
Additional side effect burden (nausea, fatigue, dizziness) in already-burdened patients
No impact on the underlying neuropathic progression
Used off-label for this indication; not FDA-approved for CIPN
PHARMACOLOGIC
Gabapentin
Off-Label, No Evidence
Widely prescribed despite no controlled evidence supporting its use in CIPN. Clinical guidelines explicitly recommend against gabapentinoids for this indication.
WHY IT FAILS
No randomized controlled trial has demonstrated efficacy in CIPN
ASCO guidelines recommend against use for CIPN prevention or treatment
Sedation and cognitive dulling impair quality of life during chemotherapy
Risk of dependence and withdrawal with prolonged use
PHYSICAL
Cryotherapy
Unproven
Ice gloves and compression socks applied during infusion to reduce drug delivery to extremities. Logistically difficult, uncomfortable, and supported by limited and conflicting data.
WHY IT FAILS
Uncomfortable for patients already enduring multi-hour infusion sessions
Limited and conflicting clinical evidence across studies
Requires in-clinic administration during every infusion cycle
No standardized protocols; wide variation in technique
Only addresses extremities, not systemic nerve damage
PHYSICAL
T.E.N.S. Therapy
Symptom Management Only
Transcutaneous electrical nerve stimulation provides temporary pain modulation by disrupting nerve signaling. It does not address nerve damage and has minimal evidence specific to CIPN.
WHY IT FAILS
Masks pain signals without treating the underlying nerve injury
Effects are temporary; symptoms return when stimulation stops
Very limited clinical evidence specific to chemotherapy-induced neuropathy
Requires patient compliance with daily electrode placement during treatment
BEHAVIORAL
Exercise
Impractical for Cancer Patients
The only approach with genuine neuroprotective evidence through mechanobiological pathways. But chemotherapy patients are too fatigued, immunosuppressed, and deconditioned to exercise at therapeutic levels.
WHY IT FAILS
Proven neuroprotective through multi-pathway mechanical signaling
Activates conserved mechanosensitive signaling pathways to protect neurons
Chemotherapy-related fatigue prevents adherence in 60-80% of patients
Not feasible at therapeutic intensity during chemotherapy cycles
PHARMACOLOGIC
Duloxetine
Off-Label, Modest Evidence
The only guideline-recommended option, but only for existing symptoms. It has never been shown to prevent CIPN, and its benefit is modest even for pain management.
WHY IT FAILS
Treats pain only; does not restore nerve function or prevent damage
Modest efficacy: NNT of ~5 for 30% pain reduction
Additional side effect burden (nausea, fatigue, dizziness) in already-burdened patients
No impact on the underlying neuropathic progression
Used off-label for this indication; not FDA-approved for CIPN
PHYSICAL
Cryotherapy
Unproven
Ice gloves and compression socks applied during infusion to reduce drug delivery to extremities. Logistically difficult, uncomfortable, and supported by limited and conflicting data.
WHY IT FAILS
Uncomfortable for patients already enduring multi-hour infusion sessions
Limited and conflicting clinical evidence across studies
Requires in-clinic administration during every infusion cycle
No standardized protocols; wide variation in technique
Only addresses extremities, not systemic nerve damage
PHYSICAL
T.E.N.S. Therapy
Symptom Management Only
Transcutaneous electrical nerve stimulation provides temporary pain modulation by disrupting nerve signaling. It does not address nerve damage and has minimal evidence specific to CIPN.
WHY IT FAILS
Masks pain signals without treating the underlying nerve injury
Effects are temporary; symptoms return when stimulation stops
Very limited clinical evidence specific to chemotherapy-induced neuropathy
Requires patient compliance with daily electrode placement during treatment
PHARMACOLOGIC
Gabapentin
Off-Label, No Evidence
Widely prescribed despite no controlled evidence supporting its use in CIPN. Clinical guidelines explicitly recommend against gabapentinoids for this indication.
WHY IT FAILS
No randomized controlled trial has demonstrated efficacy in CIPN
ASCO guidelines recommend against use for CIPN prevention or treatment
Sedation and cognitive dulling impair quality of life during chemotherapy
Risk of dependence and withdrawal with prolonged use
BEHAVIORAL
Exercise
Impractical for Cancer Patients
The only approach with genuine neuroprotective evidence through mechanobiological pathways. But chemotherapy patients are too fatigued, immunosuppressed, and deconditioned to exercise at therapeutic levels.
WHY IT FAILS
Proven neuroprotective through multi-pathway mechanical signaling
Activates conserved mechanosensitive signaling pathways to protect neurons
Chemotherapy-related fatigue prevents adherence in 60-80% of patients
Not feasible at therapeutic intensity during chemotherapy cycles
Our Solution
LIV for CIPN Treatment
LIV for CIPN Treatment
Where existing therapies have failed, LIV represents a novel therapeutic modality with numerous benefits in CIPN
Where existing therapies have failed, LIV represents a novel therapeutic modality with numerous benefits in CIPN
Learn more about how LIV activates natural mechanobiology throughout the body.
Clinical Evidence
Signals from our pilot trial in CIPN
Signals from our pilot trial in CIPN
Sham-controlled data from cancer patients with CIPN show that LIV has promise as a novel therapeutic modality for neuropathy.
Trial Design
Population
38 Cancer survivors with persistent, chronic CIPN
Intervention
12 weeks of LIV therapy (30Hz, 0.4g) vs Usual Care.
Key Takeaways:
COHEN'S D
0.45
Medium Effect
FACT/GOG-Ntx (4-item)
SENSORY NEUROPATHY SYMPTOMS
LIV Improved Sensory CIPN Symptoms
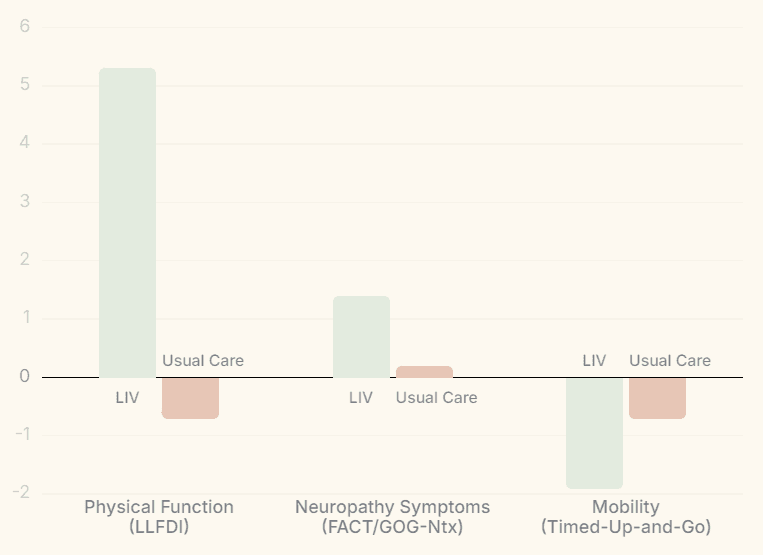
LIV participants reported greater improvement in sensory neuropathy symptoms (+1.4 points) compared to usual care (+0.2 points). The between-group difference falls within the minimal clinically important difference range, reflecting a meaningful reduction in numbness, tingling, and discomfort.
COHEN'S D
0.80
Large Effect
LLFDI Basic Lower Extremity Test
LOWER EXTREMITY FUNCTION
Large Improvements in Physical Function
LIV patients gained +5.3 points in basic lower extremity function while the usual care group declined by 0.7 points. This surpasses the minimal clinically important difference threshold and represents the study's strongest patient-reported outcome.
COHEN'S D
0.84
Large Effect
Sagittal Centroidal Frequency
POSTURAL STABILITY
Significant Ehancement of Postural Stability
Sagittal centroidal frequency (a measure of postural sway) decreased 0.15 Hz with LIV, indicating improved stability, while usual care showed no change. Reduced postural sway is directly associated with lower fall risk, a critical concern for patients with CIPN.
COHEN'S D
0.60
Medium Effect
Timed-Up-and-Go
MOBILITY
LIV meaningfully improved mobility
LIV participants improved Timed-Up-and-Go time by 1.9 seconds compared to 0.7 seconds in usual care. Gait quality also improved: LIV patients took fewer steps over 4 meters (d = 0.60) with longer step length (d = 0.43), consistent with reversal of the conservative gait pattern seen in neuropathy.
0
Serious Adverse Events
97%
Trial Retention
77%
Session Adherence
SAFETY AND FEASIBILITY
Safe, feasible, and well-tolerated in cancer survivors
No serious adverse events were reported. Trial retention reached 97% and adherence to twice-daily LIV sessions averaged 77%, confirming that brief, home-based LIV therapy is practical and acceptable for cancer survivors with persistent CIPN.
COHEN'S D
0.45
Medium Effect
FACT/GOG-Ntx (4-item)
SENSORY NEUROPATHY SYMPTOMS
LIV Improved Sensory CIPN Symptoms
LIV participants reported greater improvement in sensory neuropathy symptoms (+1.4 points) compared to usual care (+0.2 points). The between-group difference falls within the minimal clinically important difference range, reflecting a meaningful reduction in numbness, tingling, and discomfort.
COHEN'S D
0.80
Large Effect
LLFDI Basic Lower Extremity Test
LOWER EXTREMITY FUNCTION
Large Improvements in Physical Function
LIV patients gained +5.3 points in basic lower extremity function while the usual care group declined by 0.7 points. This surpasses the minimal clinically important difference threshold and represents the study's strongest patient-reported outcome.
COHEN'S D
0.84
Large Effect
Sagittal Centroidal Frequency
POSTURAL STABILITY
Significant Ehancement of Postural Stability
Sagittal centroidal frequency (a measure of postural sway) decreased 0.15 Hz with LIV, indicating improved stability, while usual care showed no change. Reduced postural sway is directly associated with lower fall risk, a critical concern for patients with CIPN.
COHEN'S D
0.60
Medium Effect
Timed-Up-and-Go
MOBILITY
LIV meaningfully improved mobility
LIV participants improved Timed-Up-and-Go time by 1.9 seconds compared to 0.7 seconds in usual care. Gait quality also improved: LIV patients took fewer steps over 4 meters (d = 0.60) with longer step length (d = 0.43), consistent with reversal of the conservative gait pattern seen in neuropathy.
0
Serious Adverse Events
97%
Trial Retention
77%
Session Adherence
SAFETY AND FEASIBILITY
Safe, feasible, and well-tolerated in cancer survivors
No serious adverse events were reported. Trial retention reached 97% and adherence to twice-daily LIV sessions averaged 77%, confirming that brief, home-based LIV therapy is practical and acceptable for cancer survivors with persistent CIPN.
COHEN'S D
0.45
Medium Effect
FACT/GOG-Ntx (4-item)
SENSORY NEUROPATHY SYMPTOMS
LIV Improved Sensory CIPN Symptoms
LIV participants reported greater improvement in sensory neuropathy symptoms (+1.4 points) compared to usual care (+0.2 points). The between-group difference falls within the minimal clinically important difference range, reflecting a meaningful reduction in numbness, tingling, and discomfort.
COHEN'S D
0.80
Large Effect
LLFDI Basic Lower Extremity Test
LOWER EXTREMITY FUNCTION
Large Improvements in Physical Function
LIV patients gained +5.3 points in basic lower extremity function while the usual care group declined by 0.7 points. This surpasses the minimal clinically important difference threshold and represents the study's strongest patient-reported outcome.
COHEN'S D
0.84
Large Effect
Sagittal Centroidal Frequency
POSTURAL STABILITY
Significant Ehancement of Postural Stability
Sagittal centroidal frequency (a measure of postural sway) decreased 0.15 Hz with LIV, indicating improved stability, while usual care showed no change. Reduced postural sway is directly associated with lower fall risk, a critical concern for patients with CIPN.
COHEN'S D
0.60
Medium Effect
Timed-Up-and-Go
MOBILITY
LIV meaningfully improved mobility
LIV participants improved Timed-Up-and-Go time by 1.9 seconds compared to 0.7 seconds in usual care. Gait quality also improved: LIV patients took fewer steps over 4 meters (d = 0.60) with longer step length (d = 0.43), consistent with reversal of the conservative gait pattern seen in neuropathy.
0
Serious Adverse Events
97%
Trial Retention
77%
Session Adherence
SAFETY AND FEASIBILITY
Safe, feasible, and well-tolerated in cancer survivors
No serious adverse events were reported. Trial retention reached 97% and adherence to twice-daily LIV sessions averaged 77%, confirming that brief, home-based LIV therapy is practical and acceptable for cancer survivors with persistent CIPN.
Development Path
A capital efficient path to FDA clearance
A capital efficient path to FDA clearance
Two decades of existing clinical evidence and a defined regulatory path compress both the timeline and the capital required to reach the market.
Two decades of existing clinical evidence and a defined regulatory path compress both the timeline and the capital required to reach the market.
~4 Years
to FDA clearance
to FDA clearance
vs. 5–7 years for a typical Class II device. Existing safety data and a streamlined regulatory path compress the timeline.
vs. 5–7 years for a typical Class II device. Existing safety data and a streamlined regulatory path compress the timeline.
~$6M
total capital to clearance
total capital to clearance
vs. $15–25M industry average. Pre-existing designation as Non-Significant Risk (NSR) reduces time and cost burden for a pivotal trial.
vs. $15–25M industry average. Pre-existing designation as Non-Significant Risk (NSR) reduces time and cost burden for a pivotal trial.
B.D.D.
designation by 2027
designation by 2027
Lahara's device meets the criteria necessary for BDD. CIPN is irreversible, with no FDA-approved prevention or treatment.
Lahara's device meets the criteria necessary for BDD. CIPN is irreversible, with no FDA-approved prevention or treatment.
2026-2027
Endpoint Selection Trial
N=30–40 patients. Validates safety, usability, and treatment parameters. Data informs pivotal trial design. Q-sub meeting with FDA in 2026.
2026-2027
Endpoint Selection Trial
N=30–40 patients. Validates safety, usability, and treatment parameters. Data informs pivotal trial design. Q-sub meeting with FDA in 2026.
2028-2029
Pivotal Trial
N=160 (80/arm). Multi-center, sham-controlled RCT covering breast cancer patients on taxane regimens. Primary endpoint: Functional testing, PROs, and dose reductions.
2028-2029
Pivotal Trial
N=160 (80/arm). Multi-center, sham-controlled RCT covering breast cancer patients on taxane regimens. Primary endpoint: Functional testing, PROs, and dose reductions.
2030
De Novo Class II Submission
Target <150 day review. Clearance enables commercial launch and sets predicate for label expansion.
2030
De Novo Class II Submission
Target <150 day review. Clearance enables commercial launch and sets predicate for label expansion.
2030
De Novo Class II Submission
Target <150 day review. Clearance enables commercial launch and sets predicate for expansion.
Market Opportunity
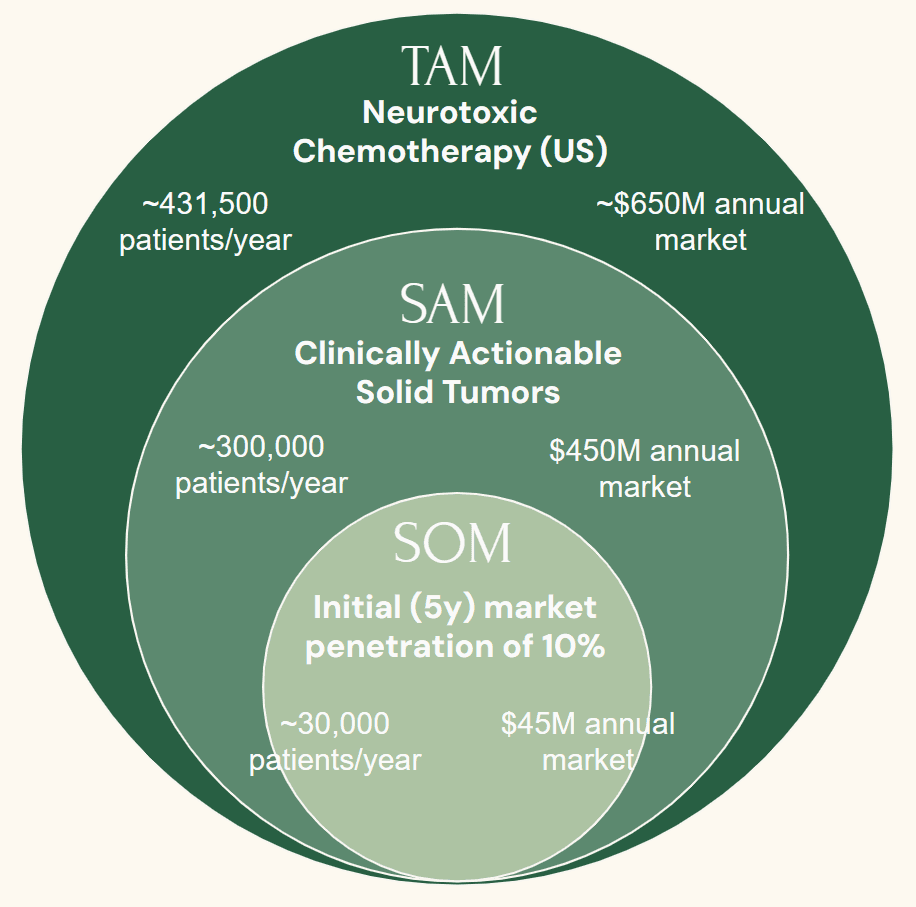
First mover in a growing market
First mover in a growing market
Zero FDA-cleared competitors. Clear reimbursement pathway. Strong payer incentive to reduce downstream costs.
Indication Expansion
A built-in platform across disease indications
A built-in platform across disease indications
LIV's conserved mechanobiological mechanism treats the same cellular pathology across multiple diseases, creating a platform with compounding clinical and commercial value at each stage.
LIV's conserved mechanobiological mechanism acts equally across multiple diseases, creating a platform with compounding clinical and commercial value at each stage.
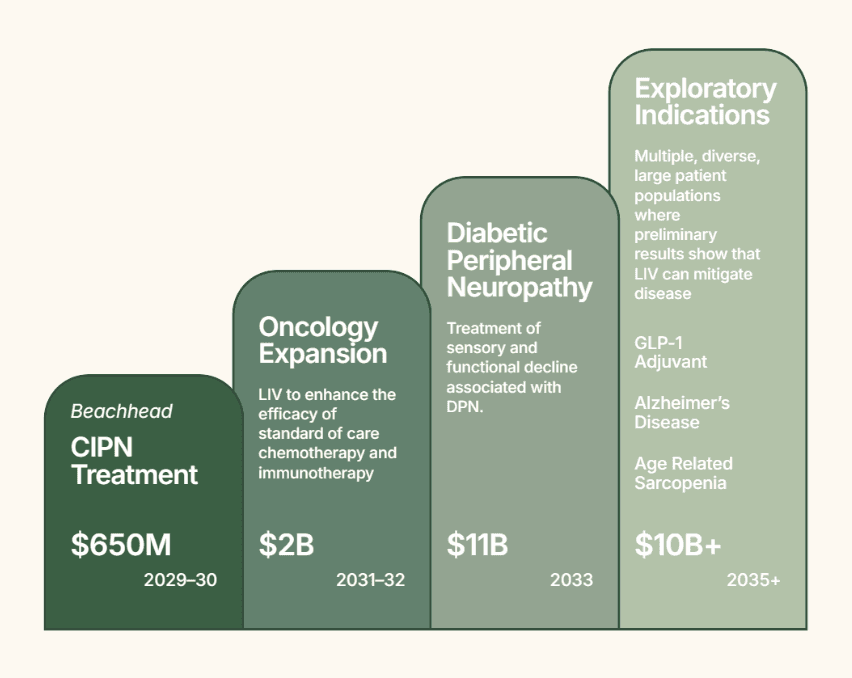
Efficient Indication Expansion.
Efficient Indication Expansion.
Each stage of development generates data that de-risks the next. The CIPN treatment trial produces safety, compliance, and mechanistic data that directly support a diabetic neuropathy filing without starting from scratch. Every CIPN patient treated alongside active chemotherapy generates real-world evidence on treatment tolerance and immune function.

